
AI Case Management
Bringing AI to Case Management — Without Taking the Human Out of the Loop

Bringing AI to Case Management — Without Taking the Human Out of the Loop
Posted by James Orr, Founder — Orracle LLC
Anyone who has worked in care coordination knows the bottleneck. A hospital discharges a patient who needs follow-up services, and a referral goes out. That referral might arrive as a fax. It might be an email. It might be a scanned PDF of a handwritten form, or a clean record from an electronic medical record system. Whatever shape it takes, a human being has to sit down, read it, pull out the details that matter, figure out how urgent it is, and get that person scheduled for care.
Multiply that by a full caseload, and you get the reality most case managers live with every day: too many referrals, too little time, and the constant worry that someone who needed help first is sitting at the bottom of the pile.
I've spent time on both sides of this problem. As a licensed clinical social worker (LCSW-S), I've done the work. As a developer, I've spent the last stretch building a tool to fix it. Today I want to share what we've built at Orracle LLC — an AI-powered, HIPAA- and FHIR-compliant case management platform designed to take the manual grind out of intake while leaving every clinical decision firmly in human hands.
The core idea: the AI proposes, the clinician decides
The single most important design principle behind this platform is that it never acts on its own. There is no scenario where the system creates a patient chart, schedules an appointment, or routes a referral without a person signing off. The AI does the heavy lifting of reading and organizing information; the human does the judging.
That distinction matters enormously in healthcare. Automation that removes human oversight is a liability. Automation that amplifies human capacity — that lets one case manager do the careful work of three — is exactly what overstretched care teams need.
What the platform actually does
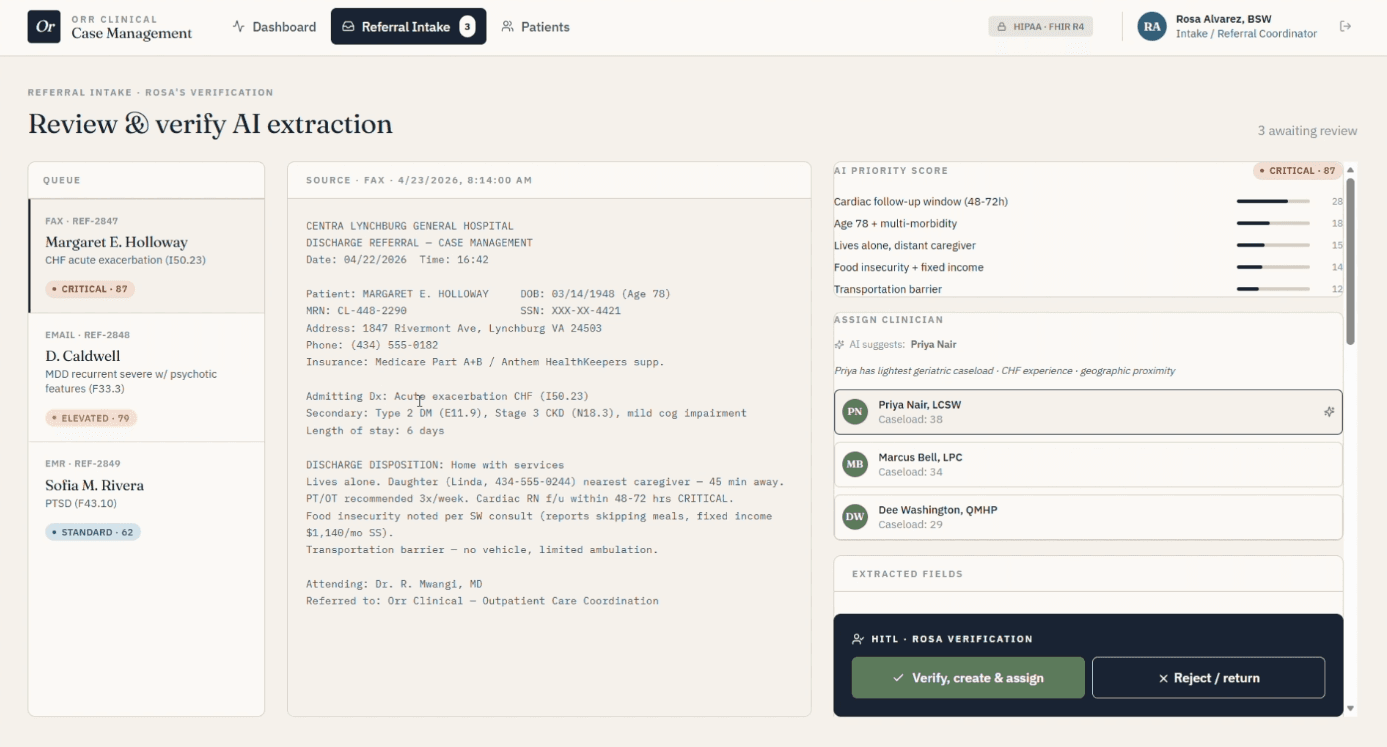
It reads any referral format. Faxes, emails, physical scans, and standard EMR referral formats all flow into the same intake pipeline. The system uses AI to extract the information that drives decisions: patient age, diagnosis, insurance coverage, distance from available services, and social determinants of health. Instead of a coordinator manually keying in fields from a blurry fax, the platform surfaces them automatically — each with a confidence score so the human knows where to look closely.
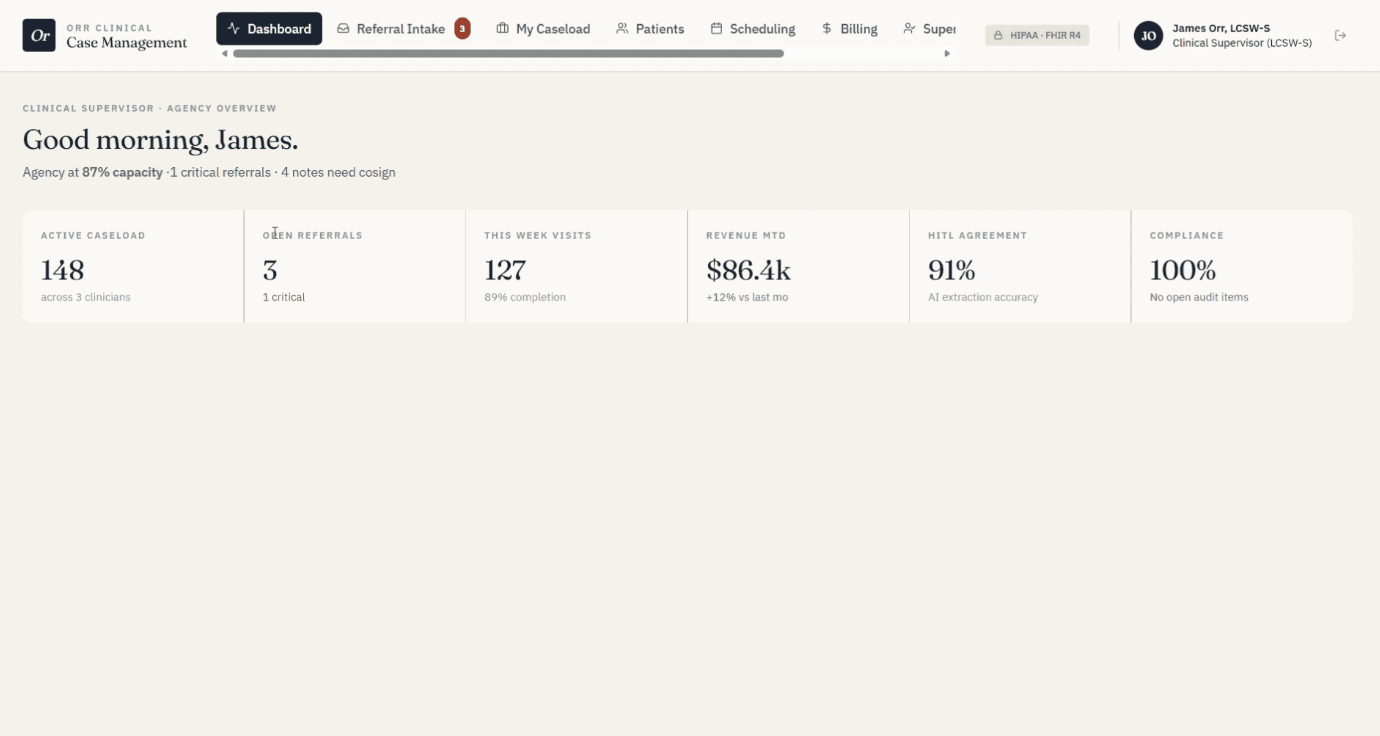
It prioritizes who should be seen first. Not every referral is equally urgent, and triage by arrival order fails the people who need help most. The platform scores incoming referrals using a combination of factors — clinical acuity, social determinants of health, insurance gaps, and barriers to access like distance — so the most vulnerable patients rise to the top of the queue rather than waiting their turn alphabetically.
It keeps a human in the loop at every gate. When a referral comes in, the AI presents its extraction and its reasoning. The coordinator reviews, edits any field that needs correcting, and only then approves the creation of a new patient chart or the merge into an existing one. The system tracks exactly which fields a human changed, which doubles as a quality signal for monitoring how well the AI is performing over time.
It supports the case manager's daily work. Once a patient is in the hub, the platform offers AI-assisted tools — risk stratification, social-determinant summaries, and next-best-action recommendations — to help case managers stay on top of their caseloads and make sure nobody slips through the cracks.
It recommends scheduling and billing — for human approval. The system can propose an appointment slot, attach the appropriate billing code, and flag the payer authorization status, all pre-filled and ready. The case manager simply verifies and confirms. The recommendation does the tedious part; the clinician owns the decision.
Built for healthcare's real constraints
This isn't a generic chatbot wrapped in a medical theme. It was architected from the ground up around the realities of clinical operations:
HIPAA-conscious by design, with the ability to run on-premises so sensitive data stays under the organization's control.
FHIR-compatible, so patient records and encounters speak the standard language of health data exchange and can integrate with existing systems.
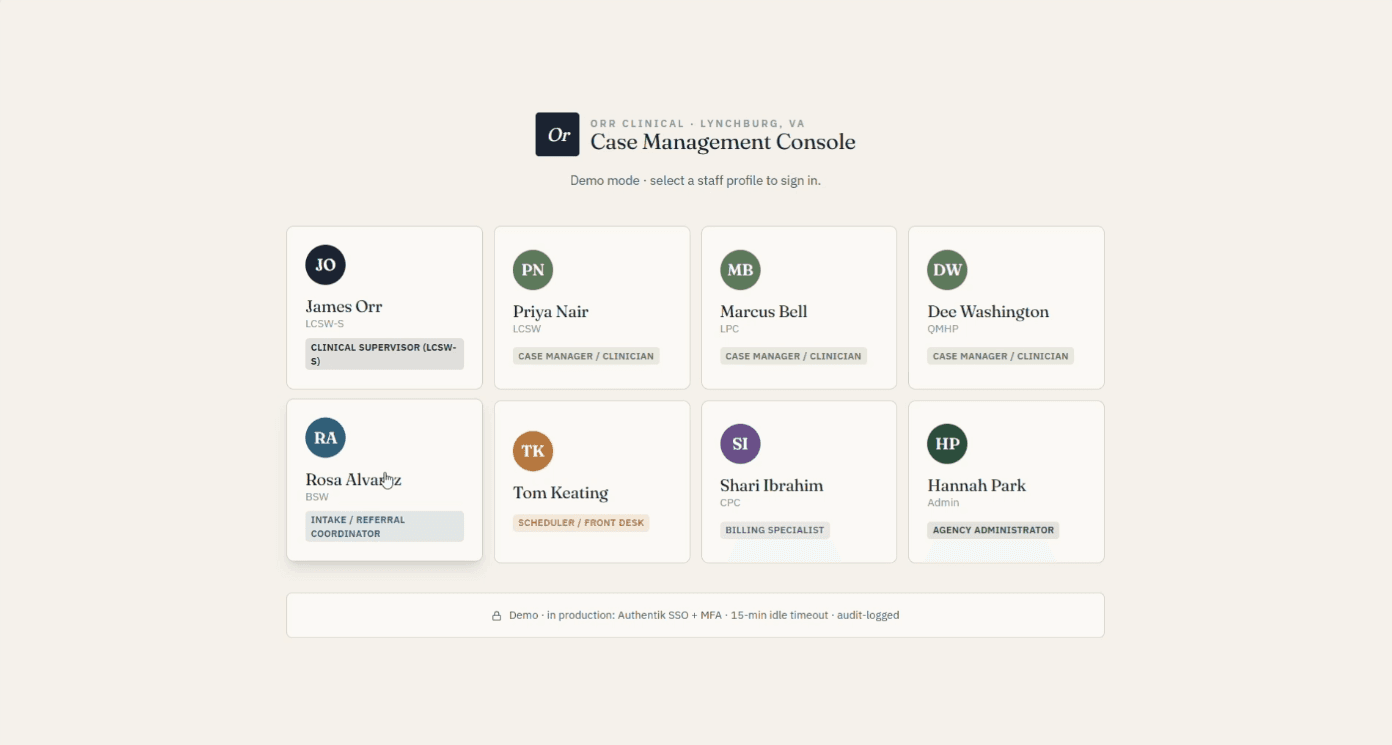
Fully audit-logged, with a complete access trail showing who did what and when.
Role-based access, with distinct permissions for intake coordinators, case managers, and clinicians, so each person sees exactly what their job requires.
Why this matters
The patients who fall through the cracks in care coordination are rarely the easy cases. They're the elderly patient with multiple conditions and no transportation. The person with a coverage gap and a new diagnosis. The family navigating a system that assumes they have the time and resources to advocate for themselves. Those are precisely the people a smarter triage and intake process is designed to catch.
I built this because I've seen the cost of the status quo, and I believe AI's role in healthcare isn't to replace the people who care for patients — it's to give them back the hours they currently lose to paperwork, so they can spend that time on the work only a human can do.
Let's talk
We have a working platform and a demo ready to share. If you're a health system, a care coordination organization, a payer, or an investor who sees where this is headed, I'd genuinely like to hear from you. Reach out through orraclellc.com — I'm happy to walk you through a live demonstration.
Orracle LLC — building responsible AI for healthcare operations.